What is AI in healthcare, in 2026?
AI in healthcare in 2026 spans 12 production categories: AI medical scribes (Abridge, Freed, Heidi, DAX), clinical decision support (OpenEvidence, UpToDate Expert AI), radiology triage (Aidoc, Viz.ai, DeepHealth), medical coding (CodaMetrix), patient triage (Infermedica, Ada), pathology (Tempus, PathAI), and seven more. 249 tools indexed, MD-reviewed, last updated July 2, 2026.
How is AI used within healthcare?
Twelve production segments group every tool we track. Each has its own MD-reviewed pillar with hand-curated picks, buyer’s guide, comparison table, and clinician FAQ.
AI medical scribes
The best AI medical scribe for most US physicians is Abridge for hospital systems, Freed AI for solo practice under $100 per month, Heidi Health for multilingual capture, and DAX C…
32 tools indexed
Decision support
Differential diagnosis, treatment guidance, drug interactions, evidence-grounded Q&A. The CDS landscape ranges from the UpToDate gold standard to physician-only OpenEvidence. We co…
18 tools indexed
Research tools
Literature search, paper summarization, citation analysis, systematic-review extraction. Consensus and OpenEvidence have absorbed most clinician research traffic in 2026. We compar…
15 tools indexed
Radiology
Acute-care triage, mammography screening, CCTA plaque analysis, mobile MRI. 30+ FDA-cleared platforms across stroke, oncology, cardiac. Enterprise sales only — we compared what's d…
33 tools indexed
Mental health
Two distinct markets in one category: provider tools (therapy-scribes, supervision AI, session analytics) and patient tools (CBT chatbots, mood trackers, AI companions). We separat…
22 tools indexed
Patient triage
Symptom checkers, voice agents, intake automation, post-discharge messaging. Tools that reduce front-desk load, improve access, and route patients to the right care setting.
19 tools indexed
Billing & coding
Autonomous coding (CodaMetrix #1 KLAS 2026), denial prevention, prior-auth automation. The single fastest path to ROI in healthcare AI is RCM — these tools deliver it.
21 tools indexed
Pathology
Digital pathology workflows with FDA-cleared cancer detection (prostate, breast, colon), IHC scoring (HER2, Ki67), and AI-powered image management. Tempus, PathAI, Proscia dominate…
17 tools indexed
Drug info
Drug references (Lexidrug, Micromedex, Epocrates), interaction checkers, and emerging AI drug-discovery platforms (Insilico, Schrödinger, Recursion). Two distinct markets covered.
14 tools indexed
Medical education
USMLE prep (UWorld, AMBOSS, Anki), specialty learning (SketchyMedical, Pathoma, Boards & Beyond), CME (Healio AI, AMA Ed Hub). The most affiliate-rich category in healthcare AI.
19 tools indexed
Surgical AI
Surgical video intelligence (Theator, Caresyntax), OR analytics (OR Black Box), VR training (Osso VR, FundamentalVR), robotic AI (da Vinci 5 Case Insights). Mostly enterprise capit…
20 tools indexed
Population health
Risk stratification, value-based care analytics, payer-side data platforms. Innovaccer #1 KLAS PHM 2026, ClosedLoop #1 KLAS Data Science. Mostly enterprise — we mapped the field.
19 tools indexed
Common questions about AI in healthcare
The answers below cover the most-googled questions for general AI-in-healthcare queries. For category-specific questions, open the matching pillar.
What is AI in healthcare?
AI in healthcare refers to clinical and administrative software that uses machine learning to perform tasks normally requiring human judgment: documenting patient encounters, surfacing differential diagnoses, reading radiology and pathology images, triaging symptoms, autonomous medical coding, drug-interaction checking, and surfacing peer-reviewed evidence. In 2026 the production-deployed segments are AI medical scribes, radiology triage, clinical decision support, medical coding, and patient triage. Other segments like surgical AI and population-health analytics remain mostly enterprise procurement.
What are AI tools in healthcare?
The current 2026 production set includes ambient AI scribes (Abridge, Freed AI, Heidi Health, DAX Copilot), clinical decision support (OpenEvidence, UpToDate Expert AI, Glass Health, VisualDx), radiology triage (Aidoc, Viz.ai, DeepHealth, HeartFlow), medical research (Consensus, Elicit, OpenEvidence, Scite), AI medical coding (CodaMetrix, Fathom Health, Nym Health), patient triage (Infermedica, Ada Health, K Health), and pathology (Tempus, PathAI, Proscia). We track 240+ tools across 12 categories; each category has its own MD-reviewed pillar.
How is AI used within healthcare?
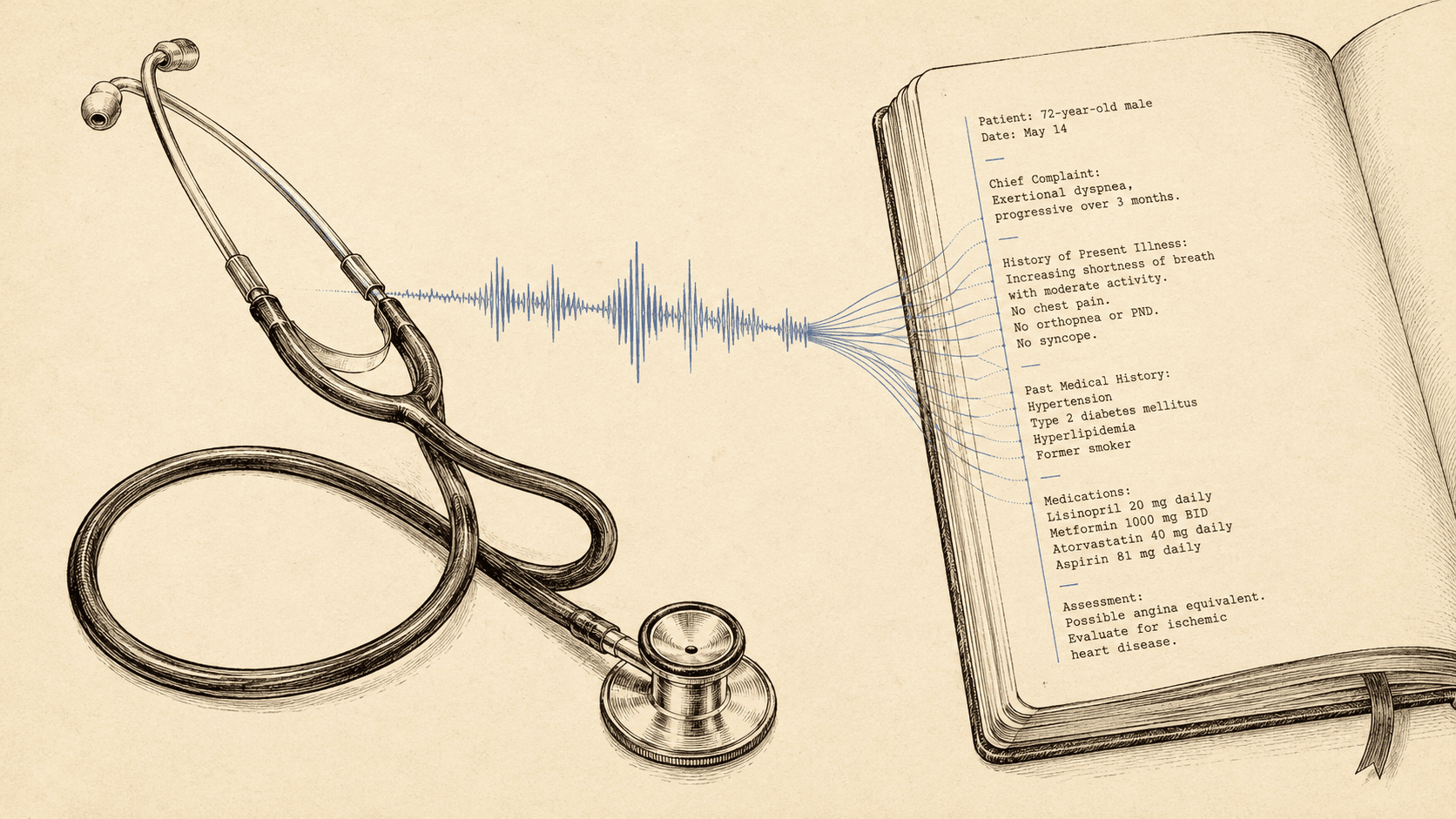
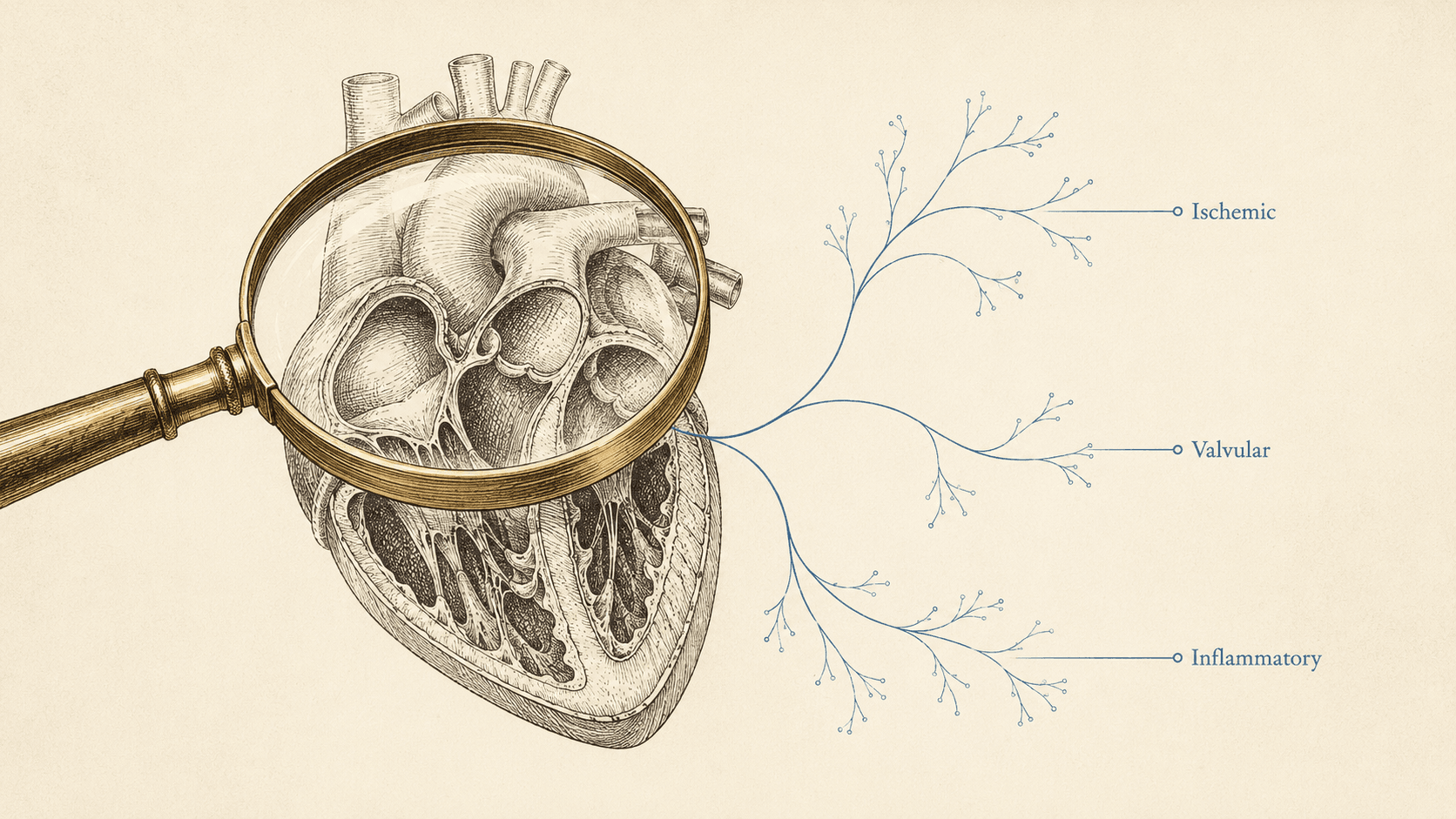
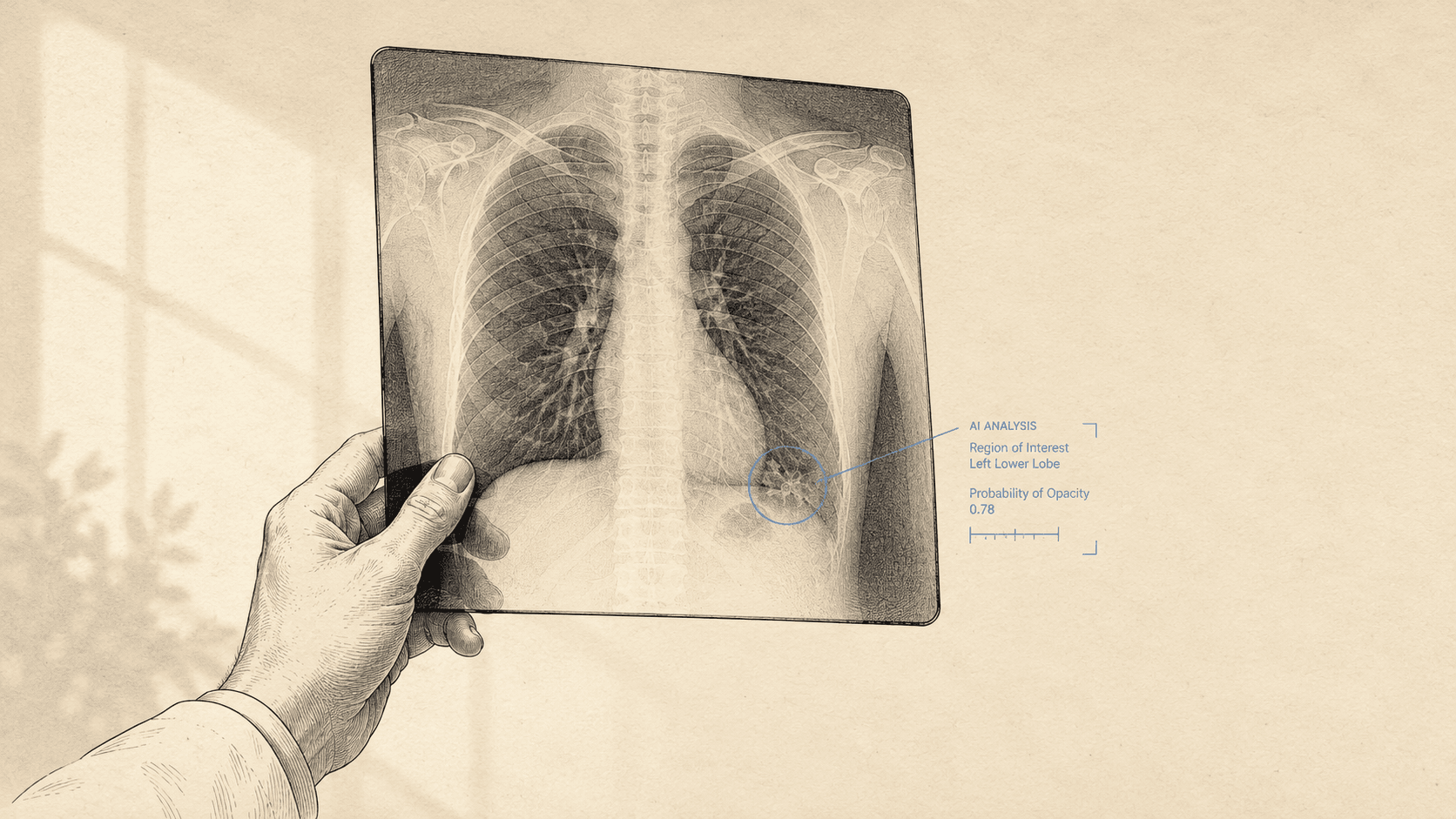
AI augments clinical workflow in five practical ways: (1) ambient documentation generates structured notes from patient-encounter audio (saves 1-2 hours per clinician per day); (2) clinical decision support answers literature-grounded questions at the point of care; (3) radiology AI triages acute findings and quantifies disease burden; (4) autonomous medical coding handles 60-90% of routine encounters; (5) patient-triage voice agents deflect non-clinical calls before they reach providers.
What are the pros and cons of AI in healthcare?
Pros: substantial time savings (1-2 hours per clinician per day on documentation), faster radiology triage, fewer missed differentials, and improved access for patients who would otherwise wait days for a callback. Cons: 2026 AI hallucination on edge cases, vendor lock-in for EHR-bundled tools, prior-authorization denials driven by payer AI, and regulatory ambiguity for tools that act as medical devices without FDA clearance. The MD-reviewed positioning we take here is that AI augments clinical workflow but does not replace clinical judgment.
What are the risks of AI in healthcare?
The clinically-relevant 2026 risks are: HIPAA non-compliance from generic LLMs used for patient-identified content (ChatGPT and Claude consumer tiers are not HIPAA-compliant out-of-the-box); hallucinated drug interactions or treatment recommendations from non-grounded models; AI prior authorization denials that increase administrative friction; and overconfidence in radiology AI outputs without radiologist sign-off. Specific FDA guidance on AI/ML-enabled medical devices is the regulatory anchor; all production tools we recommend carry explicit HIPAA attestation plus FDA 510(k) clearance where applicable.
Is there a HIPAA compliant AI tool?
Yes. HIPAA-compliant production AI tools include Abridge, DAX Copilot, Freed AI, Heidi Health, Nabla, and Suki AI for scribing; UpToDate Expert AI and OpenEvidence for clinical decision support; CodaMetrix and Cohere Health for billing and prior authorization; Aidoc and Viz.ai for radiology. Free general-purpose LLMs (ChatGPT, Claude, Gemini consumer tiers) are not HIPAA-compliant out-of-the-box and should never be used for patient-identified content.
What jobs are available in AI in healthcare?
The 2026 production hiring spans: clinical informaticists (CMIO track), AI-fluent medical coders (10-25% premium per AAPC), radiology workflow specialists, EHR integration engineers, prior-auth automation analysts, clinical AI product managers, FDA regulatory specialists for AI/ML-enabled medical devices, and AI-safety researchers focused on hallucination and bias in clinical contexts. Hiring sites: Abridge, Aidoc, Innovaccer, Tempus AI, Hippocratic AI, CodaMetrix all hire publicly.
Where can I learn AI in healthcare?
For clinician-targeted certification: Harvard Medical School AI in Health Care (online), Stanford AI in Medicine, MIT xPRO Applied AI in Medicine, Johns Hopkins AI in Healthcare specialization, and AMA Ed Hub AI modules. For self-study, follow JAMA AI, NEJM AI, and PMC NIH publications. For hands-on, OpenEvidence and Glass Health are free for verified physicians and demonstrate the production state of the field.
Will AI replace doctors?
No. The 2026 production pattern is augmentation, not replacement. AI handles narrow tasks (documentation, image triage, coding, evidence retrieval) and reduces administrative burden by 30-60% in studied workflows. Clinical judgment, complex differential reasoning, patient-relationship management, and accountability for medical decisions remain physician responsibilities. The job-displacement risk is concentrated in narrow administrative roles (parts of medical coding, basic radiology triage in some settings), not generalist clinical practice.